Spirometry is gold standard, the presence of a post-bronchod lator FEV1/FVC < 0.70 confirm the presence of persistentairflow imitation
Measurement of arterial blood gas tensions should be considered in al patients with FEV1 < 40% predicted orcinical signs suggestive of respiratory failure or rightheart failure
Reduce risk factors
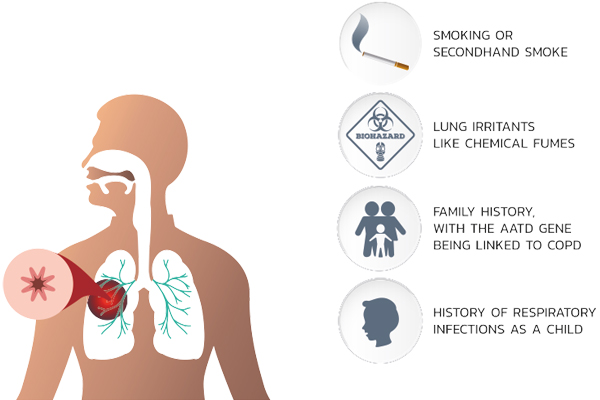
Reduction of total personal exposure to tobacco smoke, occupational custs and chemicals, and indoor air pollutants are important goals to prevent the onset and progression of COPD.
Smoking cessation is the single most effective and cost-effective way to reduce the risk of developing COPD and stop its progression
Manage stable COPD
The overall approach to managing stable COPD should be characterized by a stepwise increase in treatment, depending on the severity of the disease
Skiing can play a role in improving skills, ability to cope withiness, and health status
Bronchodilator medications are central to the symptomatic management of COPD. They are given on anes-needed basis or on a regular basis to prevent or reduce symptoms.
The principal bronchodilator is anticholinergics (SAMA & LAMA), as anticholinergic tone is high in COPD patients
Combination of different brocholitators are elective LABA&LAMA)
Regular treatment with inhaled glucocorticosteroids should only be prescribed for symptomatic patients with COPD with a documented Spirometric response to glucocorticosteroids or for those with an FEV1 <50% predicted and repeated exacerbations requiring treatment with antibiotics or oral steroids
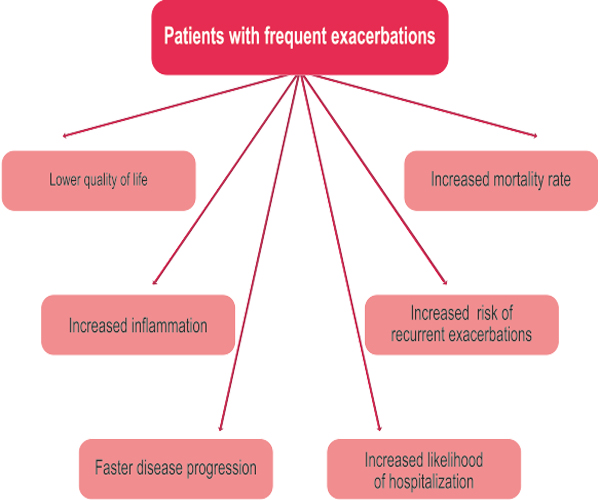
Manage exacerbations
The most common causes of an exacerbation is arpolution, but the cause of approximately one-third of severe exacerbations cannot be identified
Inhaled bronchodiators (particularly beta 2-agonists or anicholinergics)theophyline, and oral, glucocorticosteroids are efective treatment of acute Bracertations of COPD
Patients experiencing COPD exacerbations with clinical signs of airway infection 18.9., increased volume and change of color of sputum, orfever may benefit from antibiotic treatment
Nonimasive posive pressure ventilation (NIPPV) in acute exacerbations improves blood gases and pH, reduces in hospital mortality.decreases the need for invasive mechanical ventistion
Pulmonary rehabilitation
COPD patients benefit from early structured pulmonary rehabilitation program
A good nutrition programmustforal COPD patients
The long-term administration of anygen >16 h per day to patients with chronic respiratory failure has been shown to increase survival
All stable hypercapnic COPD patients benefit by long term noninvasive ventilation
Ruand pneumococcal vaccinations are beneficial to prevent exacerbation

{kind=link}